Features
Ask Dr. Craig!: Sickle Cell Disorder
 BellaNaija is pleased to announce a new column for our special readers – ‘Ask Dr. Craig!‘ Dr. Craig is a BellaNaija columnist and one of the doctors who writes for BN Doctors’ Lounge {Get familiar here}. The idea behind ‘Ask Dr. Craig!’ is for BN readers to get quick sharp answers to niggling medical issues that they have. This does not in anyway mean that readers should not go to their doctors. However, sometimes you just need a human face to give answers to those fast, burning medical concerns our readers have.
BellaNaija is pleased to announce a new column for our special readers – ‘Ask Dr. Craig!‘ Dr. Craig is a BellaNaija columnist and one of the doctors who writes for BN Doctors’ Lounge {Get familiar here}. The idea behind ‘Ask Dr. Craig!’ is for BN readers to get quick sharp answers to niggling medical issues that they have. This does not in anyway mean that readers should not go to their doctors. However, sometimes you just need a human face to give answers to those fast, burning medical concerns our readers have.
Send your questions for Dr. Craig to features(at)bellanaija(dot)com stating your full name and where you are writing from. (Your name will never be published) The editor reserves the right to edit submissions for content brevity and clarity. We regret that we cannot provide individual answers to questions sent in and cannot state at which exact date answers would be published.
We hope that people will find help by reading and sharing. We look forward to reading your emails and tweets with questions for Dr. Craig.
**
Dear Dr. Craig
Last year I met and fell in love with a wonderful woman and things have gotten quite serious between us. I have always known my genotype is AS since I was in secondary school and for this reason I made sure that I tactfully asked for the genotype of every girl I found myself interested in long before feelings got involved. This time however love snuck up on me and took me by surprise, and before I knew it I had fallen head over heels. As you have probably guessed, I just found out that the love of my life is AS too.
My heart loves her and I know she loves me in return. She is everything I have ever dreamed of and more and every day I am grateful to God for bringing her into my life. I want more than anything to spend the rest of my life with her. On the other hand my head is screaming caution! I have a close relative who has Sickle cell and I have seen what pain he has had to endure. I don’t want to have children with Sickle Cell Disease.
Is there anything that I can do?
Confused-and-in-love.
Maitama, Abuja
Dear Confused-and-in-love,
First of all, let me congratulate you on finding this kind of love that you describe. It is indeed a wonderful thing to be in love! I’m terribly sorry to hear that you are in this dilemma, but not to worry, I will do my best to provide you with all the information you need.
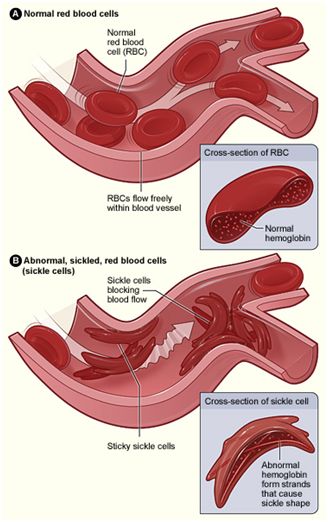
Sickle cell disorder is a blood disease that affects people of Afro-Caribbean and Asian origin and is predominant in areas that are prone to Malaria. In sickle cell disease, red blood cells that under normal circumstances can flow easily through the blood vessels tend to clump together and form abnormal shapes which restrict blood flow and can lead to vital tissues and organs being deprived of blood and oxygen.
The normal genotype AA, is responsible for the ‘doughnut’ shape of our red blood cells which makes it easy for the blood to flow through even the tiniest blood vessels. This type of blood however is very prone to severe forms of malaria. It is thought that over many years, a mutation occurred in the genes of the people living in the malaria belt and this genetic mutation conferred protection from malaria on those that had it. This mutation is the AS carrier trait. However, when two carriers marry, it was observed that while some of their children had the normal genotype AA, some had the protective mutation AS, and some others got the genotype SS and developed a condition known as Sickle cell disease.
For a couple who are both carriers of the Sickle cell trait, the probability of having a child with the normal AA genotype is 1 in 4. This means that for every pregnancy, there is a 25% chance that the child would be AA.
The probability of having a child with the carrier state genotype AS is 2 in 4. This means that for every pregnancy, there is a 50% chance that the child would be AS.
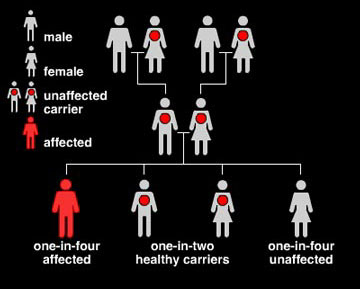
The probability of having a child with the diseased genotype SS is also 1 in 4. This too means that for every time the wife gets pregnant, there is a 25% chance that the baby would be SS.
The thing with probability however, is that it is just like throwing dice. One man can throw the dice ten times and get 6 each time, while another can throw the same dice ten times and get 1 all through. In the same way, a couple may be fortunate enough to have all their children born AA, while some will get a mixture of AA and AS or AA, AS and SS, and some also can unfortunately have all the children born to them being SS.
Counselling aims to give couples such as yourself and your girlfriend all the information that is available as well as outlining all the possible options that are open to you in a clear and unbiased way. The couple is then encouraged to carefully weigh each option with their own personal circumstances, beliefs and convictions and make a decision for themselves.
These are all the options that are available to you:
Get married and have no children
A good number of people, especially in the western world are choosing to get married and not have any children. Whereas in Africa children are seen as a completion to the marriage and are essential for keeping the family name alive, couples in Europe, Asia and the Americas are increasingly comfortable with limiting the scope of their marriage to the companionship that being together brings.
Get married and adopt
Some people choose to adopt children instead of having any of their own. Adoption is commoner in the west, and in some places like Hollywood has actually become a fad, with stars like Brangelina having adopted many children from all over the world. Adoption services are possible in Nigeria through the many orphanages here.
Get married and throw the dice
The odds of having a healthy child without any intervention are seemingly good. Three out of four. This means that there is a 75% chance that every given pregnancy could be either AA or AS. The other 25% is the likelihood of the baby being born SS. For some people these odds are good enough and they go ahead to marry and have children in the hope that the odds would be in their favour.

It is important to make clear again at this point that there will be couples who take this route and are fortunate enough to have all their children healthy (AA or AS), or have a mixture of AA, AS and SS. However, there are also couples who unfortunately go ahead to have all their children born with the disease.
Prenatal diagnosis
Some people don’t like leaving things to chance and may feel that the 25% chance of things going wrong is too much of a gamble for them. In prenatal diagnosis, the couple throw the dice but are able to know before the baby is born what its genotype will be.
Doctors are able to take some samples from your baby while still in its mother’s womb (at this stage it is called a foetus) and determine what the genotype is. There are two ways of doing this; Amniocentesis and Chorionic Villus Sampling.
Amniocentesis is a test to look at the fluid (amniotic fluid) that surrounds your baby. Amniotic fluid has cells and other substances that can give clues about the health of the foetus.
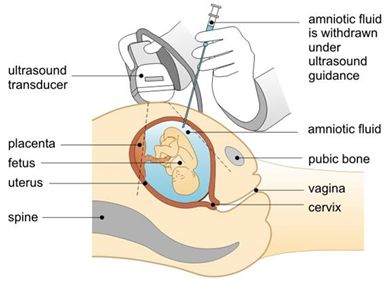
To do this a needle is gently passed through the abdomen and into the womb and a sample of the fluid surrounding the foetus is collected and is sent to the lab for analysis. Amniocentesis is done around 16 weeks of pregnancy and the results of the test can be expected at around week 20.
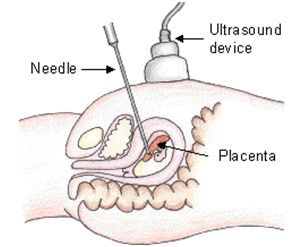
Chorionic Villus Sampling is a test done to collect samples of a tissue called Chorionic Villi from the placenta. The chorionic villi are small finger shaped projections on the surface of the placenta that have the same genetic material as those found in the foetus. To do this, a small tube is passed through the vagina and in through the cervix into the womb and small portions of chorionic villi are collected and sent for analysis. The doctor will use ultrasound to guide the tube to the right spot for collection. This can also be done by passing a needle through the abdomen. Chorionic Villus Sampling is done between the 10th and 12th weeks and results of the test can be expected at around week 14.
Prenatal diagnosis seeks to give the patients forehand knowledge of their baby’s genotype. For those whose foetus’ are diagnosed as having the SS gene, there is the option of having a Voluntary Termination of Pregnancy (VTOP). The choice of which test to use to achieve prenatal diagnosis and how quickly in the course of the pregnancy the results can be made available is important at this point, because some people find that they may need some extra time to reach a decision as to whether or not to have an abortion and the risks associated with VTOPs increase significantly the farther along the pregnancy is.
It is important to state here that not all couples decide to terminate the pregnancy, and some decide to keep the baby and go on to prepare themselves to take on whatever challenges may arise. The decision to have VTOPs is not one to be taken lightly however; as there is no guarantee as to how many VTOPs a couple may have to do before they get a positive diagnosis. The temperament of the wife, the existence of a strong support system and the convictions of the couple are all factors that need to be considered.
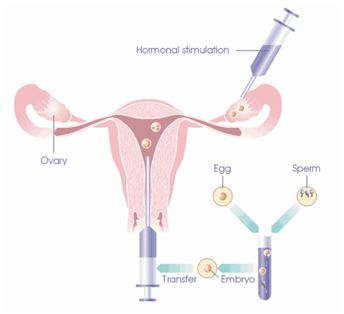
Pre implantation Genetic Diagnosis (PGD)
The aim of PGD is to ensure that couples have the best chance of having healthy children of their own. To do this the doctors will collect a number of the wife’s eggs (around 6-10) and fertilize them in the lab with her husband’s sperm (just like they do in IVF treatments). The fertilized eggs (embryos) are allowed to develop for three days and then one or two cells are removed from each embryo. The genetic material from the cells are tested and the genotype of each embryo is determined. Only those embryos that are AA are retained and the rest discarded.
Up to two AA embryos are then implanted into the wife’s womb and if the pregnancy is successful, the genotype of the baby will be AA.
So if Prenatal diagnosis allows the dice to roll and then tells you what number you have thrown, Pre Implantation genetic diagnosis ensures that your dice are programmed to throw a six every time.
This procedure for some may be quite pricey, (much more than conventional IVF) and is sadly not readily available in most centres across Africa. It is gaining widespread acceptance in most parts of Europe and in America. In some parts of Europe, however, questions have arisen about the ethical considerations attached to this procedure with the inevitable discarding of otherwise normal embryos seen as playing God and the not so distant possibility of some parents seeking to employ PGD to determine the colour of their son’s eyes or the size of their daughter’s hips.
Break up
For some couples, the amount of time, energy, emotions and finances required to have healthy children is seen as too demanding. They opt to go their separate ways and try to find love elsewhere.
I would advice that you and your girlfriend both examine these six options thoroughly and maybe do some of your own research on them as well. Send her the link to this article and schedule some alone time where you both can have an honest and open discussion on what would be best for you both as well as your future children.
For more information contact: Sickle Cell Foundation, Lagos Nigeria. www.sicklecellfoundation.com
Disclaimer: This column is written for patient education. It is not intended to diagnose or prescribe treatment and does not replace the advice of your physician. It in no means attempts to cover the full medical scope of this condition.
Photo Credit: nhlbi.nih.gov| factsanddetails.com | midlamminiatures.co.uk | orgsites.com | sogi.net.au |ramsayhealth.co.UK | cervif.com
__________________________________________________________________________________________________
David Olamide Craig is a Physician, Pastor, Photographer, Poet and Playwright. He graduated Bachelor of Medicine and Bachelor of Surgery from the University of Ibadan and holds a Masters in Occupational Health from the Institute of Occupational and Environmental Medicine, University of Birmingham. He is passionate about healthy living and sustainable energy. When he is not seeing patients, Dr. Craig spends his time stretched out on his favourite couch, reading books, magazines, and blogs. Find him on Twitter @RevDrCraig






















