Features
Ask Dr. Craig!: Rhesus Incompatibility
 Dr. Craig is a BellaNaija columnist and one of the doctors who writes for BN Doctors’ Lounge {Get familiar here}. The idea behind ‘Ask Dr. Craig!‘ is for BN readers to get quick sharp answers to niggling medical issues that they have. This does not in anyway mean that readers should not go to their doctors. However, sometimes you just need a human face to give answers to those fast, burning medical concerns our readers have.
Dr. Craig is a BellaNaija columnist and one of the doctors who writes for BN Doctors’ Lounge {Get familiar here}. The idea behind ‘Ask Dr. Craig!‘ is for BN readers to get quick sharp answers to niggling medical issues that they have. This does not in anyway mean that readers should not go to their doctors. However, sometimes you just need a human face to give answers to those fast, burning medical concerns our readers have.
Send your questions for Dr. Craig to features(at)bellanaija(dot)com stating your full name and where you are writing from. (Your name will never be published) The editor reserves the right to edit submissions for content brevity and clarity. We regret that we cannot provide individual answers to questions sent in and cannot state at which exact date answers would be published.
***
Dear Dr. Craig
I read your article on Sickle Cell Disease and was very impressed by the simplicity and ease with which you detailed the options available to couples who both have the AS genotype. I and my boyfriend at the time (now fiancé) read it and decided to get our genotypes checked and found out that we are both AA. (Yay!)
However, we also ran a couple of other tests and while the nurse assured us that all the others were okay, she mentioned that our “Rh” blood groups were incompatible and that we should come back to see the doctor for explanation.
Rh??? I thought it was only AS and SS we had to be worried about!
Please what is this Rh blood group and I hope the options available are not as expensive or as heartbreaking as those that AS/AS couples face?
(p.s Please nobody should tell me I have to look for another man o, ehen. Because I don’t think I can live without my boo and there are no men left in Lagos anyway.)
My-boo-and-I-forever. Agungi, Lagos
—–
Dear Miss My-boo-and-I-forever,
First of all, congratulations on your engagement!
I’m happy to hear that you and your fiancé found the article on Sickle Cell useful and that you have both decided to spend the rest of your lives together.
So, there’s good news and there’s not-so-good news.
-The not-so-good news is that your nurse was right. There is such a thing as the Rh (Rhesus) blood group and couples who are incompatible stand a chance of having a child that is either stillborn or born severely ill.
-The good news is that preventing the complications that can occur as a result of Rhesus incompatibility are very simple and relatively very affordable.
Before we talk about the prevention of Rhesus disease of the newborn, let’s quickly look at what causes it in the first place.
The Immune System: Antigens and Antibodies
Our bodies have a sophisticated network of defence systems that protect us from infection and disease and one of the most important of these is our immune system. The immune system is a combination of cells and chemicals and signals and receptors that help to keep our body free from invasion and infection by parasites bacteria and viruses.
So how does the immune system work?
Our immune system is so effective because it can distinguish between cells that belong to us and cells that are foreign. The default setting in our bodies is to attack and destroy all foreign cells because the body automatically assumes that they are likely to be bacteria or viruses or parasites.
When a person is exposed to a bacteria virus or parasite for the first time, the body recognises the foreign cell and immediately dispatches fighter “spy” cells to ‘learn’ how to kill the invader. These spy cells look for particles on the surface of the invading cell that they can exploit as a gateway to destroy it. These particles are called Antigens. Once the spies identify a weakness in the invaders biochemistry, they signal the barracks (bone marrow) to begin a full scale production of targeted missiles specially designed to destroy the invader. These “missiles” are Antibodies. The bone marrow also begins an intense training of specialised commando killer cells specific for the identified invader (white blood cells known as Activated T-cell lymphocytes) who will assist in the ground offensive.
Once the threat is eliminated, the antibodies remain in the body on alert and if the same invader enters the body again, they will be ready to seek out and destroy it.
Antigens are not just present on germs and parasites. In fact practically every cell including human cells have antigenic particles on their surfaces too. The difference is that the body recognises your antigens and does not attack them.
The red blood cells in our bodies have a vast range of antigens on their surface and these antigens are classified according to different groups. The most common of these are the A, B, AB and O blood groups that most people are familiar with. These antigens are particularly important when it comes to blood transfusions because the foreign blood cells could trigger the patient’s immune response. This is why before a person receives blood the doctors run a grouping and crossmatch test to ensure that the patient’s body does not have antigens in their blood that will attack and destroy the donor’s blood.
The Rh blood grouping system is a way of classifying a different group of antigens that are present on the red blood cells of humans and these are called the Rhesus antigens. There are three rhesus antigens but the one that has the most clinical significance is the Rhesus D antigen.
If a person’s red blood cells have the Rh D antigen on its surface then they are positive (+) and if they don’t have it they are negative (-).
What this means is that if a person without the antigen (-), comes in contact with blood that carries the antigen (+), their body will identify those (+) cells as foreign and destroy them.
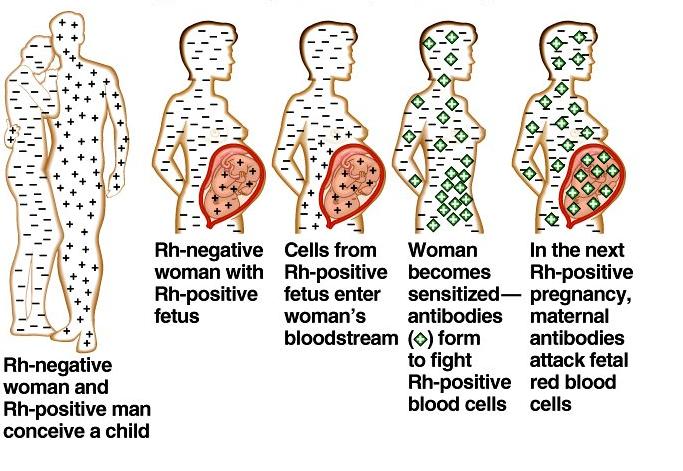
If a woman who is Rh (-) marries a man who is Rh(+) and gets pregnant, there is a tendency that her baby would inherit the Rh(+) antigen from its father. When this happens, the mothers body will identify the baby’s blood as foreign cells because the Rh(+) antigen is not present in her own body. As soon as the baby’s cells come in contact with the mother via the placenta (or during the course of delivery) the mothers body dispatches the “spy” cells to identify the antigen on the baby’s cells and signals the bone marrow to produce antibodies to destroy them. The first pregnancy usually does not have any problems because the “missiles” and “commandos” are still in production and training, but as soon as the woman gets pregnant again with another Rh(+) baby, her immune system kicks in and begins to attack the “foreign” cells in her womb. Depending on how aggressive the immune response is, the mother’s body could completely kill off her own baby or at best the baby could be born severely ill.
This is what we mean by Rhesus incompatibility
Prevention of Rh Disease of the new born
Rh (-) women can marry Rh(+) men and have healthy babies but they must receive an injection to inactivate the Rh (+) cells as soon as any event occurs that may cause the baby’s blood to mix with the mothers blood before the immune response is activated. The scenarios that can make baby’s blood come in contact with mother’s blood are:
1. Miscarriage
2. Termination of pregnancy
3. Bleeding during pregnancy (Placenta Previa /Abruption of Placenta)
4. Any testing that involves taking a sample from the baby while still in the womb (i.e. Chorionic Villous Sampling (CVS) or Amniocentesis)
5. Vaginal delivery
6. Traumatic Caesarean section delivery
Prevention of the initiation of the immune response is critical because once it occurs the antibodies will remain in the woman’s body indefinitely and will attack all subsequent pregnancies that are Rh (+). Note that if a woman is Rh(+) there is no risk of Rhesus disease of the new born since her body already has Rh antigens and would not recognize it as foreign if her baby has it too
Treatment of Rh Disease of the new born
As with all things, prevention is better than cure.
The treatment for babies whose mother’s immune systems have launched an attack on their blood cells is intense and can easily be avoided.
Babies suffering from Rhesus Disease will need to have frequent blood transfusions while still in the mother’s womb. This is done by passing a needle into the baby’s heart through the mother’s womb under ultrasound guidance or through a vein in the umbilical cord. Depending on the severity, these transfusions may have to be repeated as often as every 7-10 days.
In severe cases, as soon as the baby reaches 34 weeks, the doctors may take the decision to deliver the baby prematurely and remove it from the continued attack of the mother’s immune system.
So you see, it is perfectly safe for you to go ahead and marry your fiancé but it is very important that you let your doctors know your full and complete past obstetric history so as to give them all the information necessary to adequately prepare for you when you choose to get pregnant.
I hope this helps put your mind at ease and I wish you and your “boo” all the best with everything.
***Disclaimer: This column is written for patient education. It is not intended to diagnose or prescribe treatment and does not replace the advice of your physician. It in no means attempts to cover the full medical scope of this condition.
Photo Credit: http://i44.tinypic.com/hs6s0g.jpg





















